Variations in forearm tendons – A clinical-anatomical guide
Sie sind bereits registriert?
Loggen Sie sich mit Ihrem Universimed-Benutzerkonto ein:
Sie sind noch nicht registriert?
Registrieren Sie sich jetzt kostenlos auf universimed.com und erhalten Sie Zugang zu allen Artikeln, bewerten Sie Inhalte und speichern Sie interessante Beiträge in Ihrem persönlichen Bereich
zum späteren Lesen. Ihre Registrierung ist für alle Unversimed-Portale gültig. (inkl. allgemeineplus.at & med-Diplom.at)
Anatomical variations of the muscles and tendons of the forearm and hand are both common and significant in daily clinical practice. The flexor muscles, specifically the palmaris longus (PL) and flexor carpi radialis (FCR), are frequently utilized in reconstructive procedures for ruptured tendons and torn ligaments.1 Examples of such procedures include the reconstruction of flexor tendons, the ulnar collateral ligament, and the dorsal scapholunate ligament in cases of scapholunate dissociation.2–4
Keypoints
-
The palmaris longus (PL) was present in 74% of all examined specimens. Specifically, 64% exhibited bilateral PL, while 10% had unilateral PL, and 26% showed agenesis of the PL. Female and male PL distributions were similar, with notable variations in occurrence and structure across different populations. Awareness of these anatomical nuances is crucial for surgical planning and diagnosis.
-
The flexor carpi radialis (FCR) is not only vital due to its potential use as a tendon graft but also serves as a reliable landmark for surgical approaches to the forearm and wrist. Despite its consistent insertion onto the trapezial ridge, its insertion can also variably attach to several structures like the trapezium, the annular ligament, scaphoid, and metacarpal bases.
-
The presence of the PL muscle shows significant variability based on sex and laterality. It is more commonly absent in females and on the left side. Awareness of these trends can assist in surgical planning and patient counseling.
-
Different tendon and muscle variations, including PL configurations and FCR insertions, can affect the harvesting length, width, and structural integrity of tendons used in transplants.
The presence of different tendon variations can complicate tendon harvesting and potentially compromise the success of the procedure. Additionally, the variability in the anatomical structures around the PL and FCR tendons can pose risks to neurovascular structures during surgery, thereby necessitating careful preoperative planning and precise surgical techniques to avoid complications.
The palmaris longus (PL) muscle, in particular, exhibits the most frequently described anomalies. Variations include duplication, bifurcation, reversal, central location, division with an ulnar slip, and hypertrophy. Some reports have even depicted an anomalous PL with three heads or as three distinct muscles.5 Equally variable are the insertion sites of the PL, ranging from various muscular and osseous insertions to a doubled distal insertion, also known as the palmaris longus bicaudatus of Gruber.6 Reimann et al. reported that the PL is absent in 12,8% of the donors,7 more commonly in females and on the left side in both sexes.6
The flexor carpi radialis (FCR) is another vital forearm muscle, used for tendon grafts in hand surgery and serving as a consistent landmark for surgical approaches to the forearm and wrist. Yeager et al. observed a consistent insertion of the FCR onto the trapezial ridge in all donors,8 whereas Akita et. al. described the FCR insertion as more variable, most commonly partially or totally attached to the trapezium, but also, to the annular ligament, scaphoid, and the bases of the third and fourth metacarpals. The FCR can sometimes be duplicated or absent, with various muscular variations reported.6
Understanding the anatomical complexity of the forearm’s flexor tendons, specifically the PL and FCR, is crucial, as they are often used for tendon transplants in hand surgery.1 Given the numerous anatomical variations, this study aimed to provide a comprehensive overview of these variations, highlighting their clinical significance and implications for surgical planning in orthopedic and reconstructive procedures. The PL and FCR muscles and tendons were examined to outline the length and width of the tendons, the variability of the muscles relative to other muscles and neurovascular structures, and their relationship to the flexor retinaculum.
Results
The PL was present in 74% of all donors, with 64% having a bilateral PL, 10% a unilateral PL and 26% showing agenesis of the PL. When comparing between the sexes, 12 females (63% of all female and 39% of all donors) and 8 males (67% of all male/26% of all donors) showed a bilateral PL, 3 females (16% of all female/ 10% of all donors) and 3 males (25% of all male/10% of all donors) had a unilateral PL. The tendon length, which could have been harvested (between the most distal muscle fibers and the insertion in the palmar aponeurosis) was approximately 13cm (SD = 3cm, range = 4–19cm).
The normal PL muscle origin was the medial epicondyle (ME) and the insertion was the palmar aponeurosis and the transverse carpal ligament. The PL tendon had a round structure in 44 cases (96% of all PL/71% of all donors) and a flat, aponeurotic structure (width more than 1cm) in 2 cases (4% of all PL/3% of all donors). The PL inserted radial in 45 cases (98% of all PL/ 73% of all donors), only in one case (2% of all PL/2% of all donors) the PL inserted ulnar into the transverse carpal ligament. Furthermore, we assessed the course/location of the PL insertion with respect to the thenar muscles, and described three types – volar to thenar, into thenar and deep to thenar. In the majority of 30 cases (65% of all PL/48% of all donors) the PL inserted volar to the thenar muscles, in 12 specimens (26% of all PL/19% of all donors) the PL inserted into the thenar and in 4 cases (9% of all PL/6% of all donors) the insertion of PL was located deep to thenar.
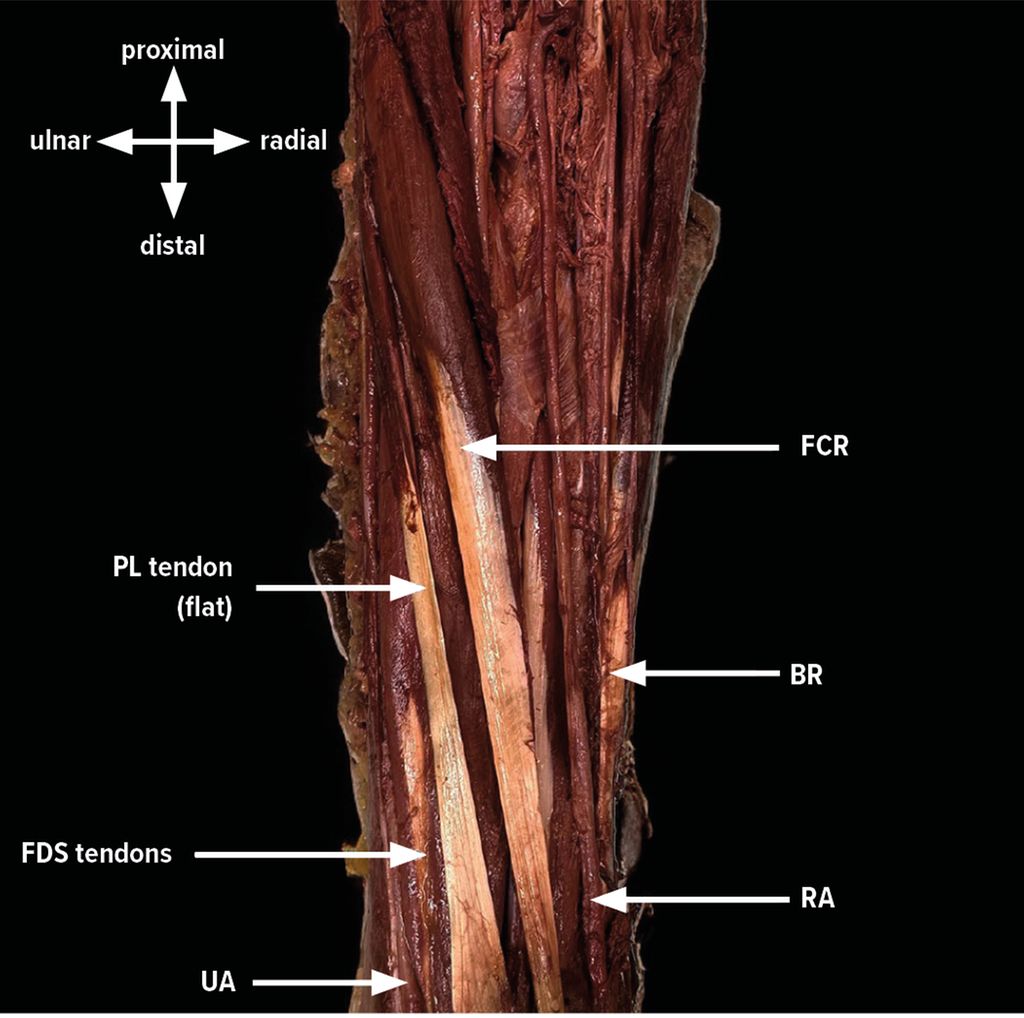
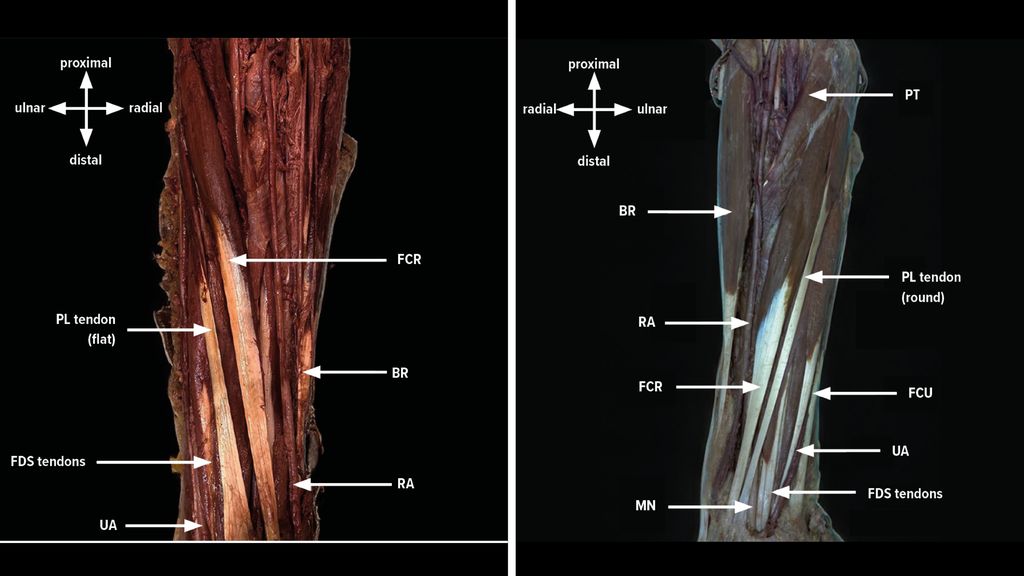
Abb. 1: Palmaris longus (PL) with a flat, aponeurotic tendon structure
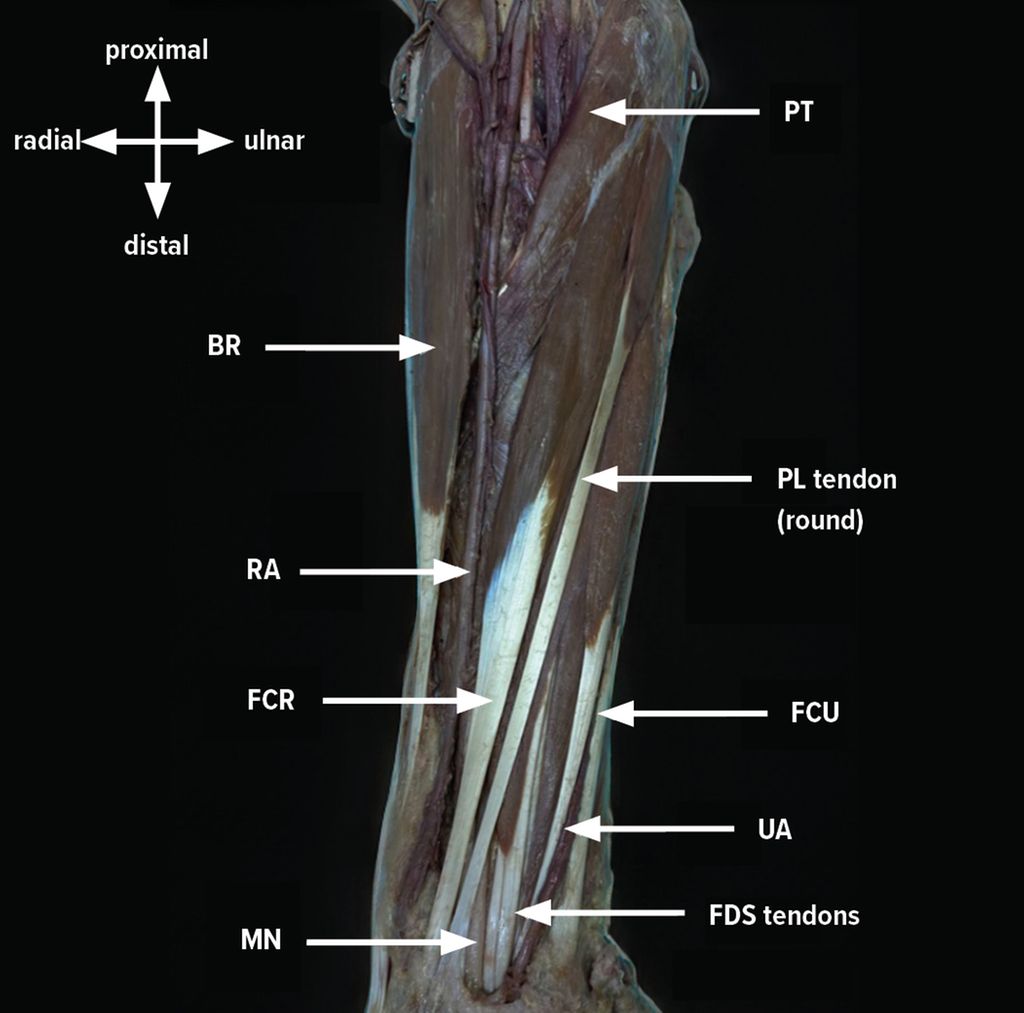
Abb. 2: Palmaris longus (PL) with a long, round tendon structure
The PL tendon showed a bifid variation in 6 cases (13% of all PL/10% of all donors), splitting between 1 to 4,5cm before inserting in the palmar aponeurosis, a trifid and multifid variation were not seen.
One case (2% of all PL/2% of all donors) showed a central muscle belly, a proximal tendon and a distal bifurcated tendon forming the PL.
In one case (2% of all PL/2% of all donors) the ulnar artery (UA) overcrossed the PL, resulting in a possibly more difficult and hazardous procedure of tendon harvesting.
FCR was present in all specimens. The distance between the most distal muscle fibers and the transverse carpal ligament was 8cm (SD= 2cm, range = 5,5–11,5cm). There were antebrachial connections in 35 cases (56%), which often consisted of muscle strands to PT and/or to FDS in the proximal third of the forearm. In 10 cases (16%) the FCR had a muscular connection to the FDS, in 15 cases (24%) to FDS and pronator teres (PT) and in 10 specimens (16%) only to PT in the proximal third of the forearm.
Discussion and conclusion
Different tendon variations can compromise the optimal length or width for tendon harvesting, result in poor tendon structure, or even endanger neurovascular structures due to anatomical differences around the flexor muscles. The literature reports a prevalence of PL in 50% to 90% of the population, with bilateral PL observed in 62,2% and unilateral PL in 15%.6,9–11
Furthermore, a reversed PL can potentially compress the median nerve (MN) at the wrist, as described by Meyer et al., although this variation was not observed in our study.13 A rare and critical variant to note is the superficial ulnar artery (SUA), which courses over the PT, FCR, and PL muscles before entering the Guyon’s canal.14
In our case, the UA ran deep to the FCR muscle, becoming superficial radially and crossing over the PL. According to Hanada et al., the SUA can be damaged during surgery, and the broad tendon of the PL might not be suitable as a tendon graft.15 Preoperative ultrasound visualization can help identify variations in either muscles or neurovascular structures. These findings can guide surgeons in understanding anatomical variations of the flexor tendons and the associated potential risks during tendon harvesting or other reconstructive procedures in this area.
Literatur:
1 Yammine K, Erić M: Morphometric analysis and surgical adequacy of palmaris longus as a tendon graft. A systematic review of cadaveric studies. Surg Radiol Anat 2020; 42(3): 259-67 2 Peters T et al.: Reconstruction of flexor pollicis longus tendon with palmaris longus interposition graft: results in 14 patients. Acta Orthop Belg 2022; 88(4): 757-60 3 Erickson BJ et al.: Ulnar collateral ligament reconstruction: anatomy, indications, techniques, and outcomes. Sports Health 2015; 7(6): 511-7 4 Erdag Y, Pehlivanoglu T: Dorsal scapholunate ligament reconstruction by using palmaris longus tendon graft in chronic static scapholunate dissociations: Does it yield favorable radiographic and functional results? J Wrist Surg 2023; 12(4): 345-52 5 Allahham S et al.: A rare anatomical finding of undescribed accessory palmaris longus in the distal forearm: A case report. Plast Reconstr Surg Glob Open 2022; 10(4): e4240 6 Akita K, Nimura A: Forearm muscles, in Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation. 2016; 298-314 7 Reimann AF et al.: The palmaris longus muscle and tendon. A study of 1600 extremities. Anat Rec 1944; 89(4): 495-505 8 Yeager K et al.: Flexor carpi radialis tendon insertion onto the trapezial ridge: An anatomic description. J Hand Surg Glob Online 2023; 5(1): 55-7 9 Yammine K, Erić M, Assi C: Variations and morphometrics of palmaris longus in fetuses: a meta-analysis of cadaveric studies. Surg Radiol Anat 2020; 42(3): 281-7 10 Kikano R et al.: Prevalence, variants, and morphometrics of palmaris longus tendon: a magnetic resonance imaging study. Surg Radiol Anat 2021; 43(5): 749-53 11 Olewnik L et al.: Anatomical variations of the palmaris longus muscle including its relation to the median nerve - a proposal for a new classification. BMC Musculoskelet Disord 2017; 18(1): 539 12 Olewnik Ł et al.: Morphological variability of the palmaris longus muscle in human fetuses. Surg Radiol Anat 2018; 40(11): 1283-91 13 Meyer FN, Pflaum BC: Median nerve compression at the wrist caused by a reversed palmaris longus muscle. J Hand Surg Am 1987; 12(3): 369-71 14 Sakulsak N, Phuapittayalert L: An unusual topographic relationship between high origin of superficial ulnar artery and bitendinous palmaris longus. Anat Sci Int 2021; 96(4): 577-81 15 Hanada M et al.: Non-anatomical reconstruction of lateral ulnar collateral ligament of the elbow after tumor resection. Strategies Trauma Limb Reconstr 2015; 10(3): 195-9
Das könnte Sie auch interessieren:

Der freie mikrovaskuläre SCIP zur Radialis-Hebedefektdeckung
Der freie Radialislappen ist insbesondere in der Kopf-Hals-Chirurgie ein bewährter Standard zur Rekonstruktion. Trotz seiner Vorteile bleibt die Versorgung der Lappenentnahmestelle am ...

Lebensqualität durch minimalinvasive funktionelle Gaumenrekonstruktion
Die funktionelle Rekonstruktion im Kopf-Hals-Bereich zählt zu den anspruchsvollsten Aufgaben moderner Chirurgie, da sie zentrale Lebensfunktionen unmittelbar betrifft. Wenn der weiche ...

Einblicke in die Geschichte des Botulinumtoxins
Die Geschichte der Entstehung des Botulinumtoxins ist bemerkenswert: Vom gefürchteten Lebensmittelgift entwickelte es sich zu einem etablierten, weltweit eingesetzten Arzneimittel mit ...