
Epigenetic and inflammatory markers in elderly cancer patients
Easy-to-measure markers to predict the incidence and course of malignancies could significantly benefit patient treatments and outcomes, specifically in the elderly patient population. Here, we discuss the current evidence of epigenetic and inflammatory markers in elderly patients with cancer and potential clinical applications.
Keypoints
-
An otherwise unexplained inflammatory state should prompt the search for an underlying malignancy.
-
While the lack of specificity of inflammatory markers limits their use, particularly in elderly patients with comorbidities, specific indicators or scores in patients may rightly be surrogate markers of disease activity over time.
-
Epigenetic and inflammatory markers cross roads in clonal hematopoiesis and leukemia, which can serve as a model to further study the intricate interplay between these two emerging hallmarks of cancer.
Altered inflammation is an emerging hallmark of cancer, and decoding epigenetic changes conferring malignancy has significantly advanced our understanding of cancer initiation and maintenance over the last few years. Both biological processes have been characterized as key drivers in various malignancies, with most cancers having the greatest incidence in elderly patients (generally defined as 65 years of age or older), where inflammation plays a key role in a process referred to as inflammaging. These elderly patients often have comorbidities limiting intensive treatment options, while disease biology can be more aggressive. The ability to measure markers to predict disease course and identify patients at risk for accelerated aging and subsequent frailty greatly facilitates decision-making. Preventive screening leveraging informed testing for epigenetic and inflammatory markers would even benefit a more significant population.
Here, we discuss current concepts and evidence on epigenetic and inflammatory markers in elderly patients using the hematopoietic system as an example of the interplay between epigenetic aberrations and inflammation.
Epigenetic markers
The regulation of oncogenic gene expression by epigenetic factors has recently been added to the list of hallmarks of cancer.1 Accumulating evidence over the last two decades has demonstrated that epigenetic regulators are commonly mutated or deregulated in cancer, leading to an aberrant activation or repression of their targets. Leukemias are a prominent example of cancers with high rates of mutations in epigenetic regulators. Among these are histone methyltransferases (e.g.,KMT2A fusions, EZH2), histone acetylases (e.g. KAT6A, p300), DNA methylases (e.g.,DNMT3A) and many more. The discovery of these oncogenic chromatin regulators has spurred the development of molecules targeting their function or chromatin binding capacity.
While there are these known associations, clinically applicable measures to determine epigenetic changes at premalignant or early stages of disease are lacking. However, monitoring peripheral blood cells bearing an alteration in epigenetic regulators can be an elegant strategy, which will be discussed below.
Inflammatory markers
It has been widely demonstrated that aging in humans (and mice) is associated with increased systemic inflammation, referred to as “inflammaging”. This chronic state of inflammation is mediated by elevated levels of circulating pro-inflammatory cytokines, including IL-1β, IL-6, TNFα, RANTES, and others.2 Moreover, it is well described that chronic inflammation is harmful to hematopoietic stem cells (HSCs)2–5 while creating an environment that offers a selective advantage to HSCs with a somatic mutation defining clonal hematopoiesis (CH), facilitating their clonal expansion.3 This connection between CH and age-related inflammation links the condition to various age-associated diseases, including cardiovascular disorders and myeloid malignancies.4,5
Even before this intricate interplay between inflammation, aging, hematopoietic cells, and major producers of inflammatory chemokines and cytokines had been characterized in greater detail, several efforts aimed to measure serum levels of cytokines, soluble receptors and putative surrogate markers of inflammation, including IL-6, IL-8, TNFα, C-reactive protein (CRP), some of which have also been shown to be correlated amongst each other.6–9 The subsequent discussion will focus on the role of inflammatory markers in older cancer patients.
Most studies to date describe associations between elevated cytokine levels, cellular surrogate markers of inflammation or their combination and malignancies. The goals of these studies were either to identify biomarkers to predict the incidence of a specific cancer type or to risk-stratify patients with a confirmed diagnosis, thereby specifically testing cancer-associated accelerated aging or frailty.
Predicting cancer
In a review of 189 studies, IL-6 levels were generally higher in patients with cancer than in healthy individuals,8 but the data did not allow for definitive conclusions. A meta-analysis on the association of circulating CRP and IL-6 levels in prospective cohorts, including older women, found an association between increased CRP and overall cancer risk and lung cancer, and weaker associations with colorectal and breast cancer; IL-6 was associated with increased lung and breast cancer.6 In a study with a median patient age of 65 years, Pine and colleagues tested the association between circulating IL-6, IL-8, and CRP in patients with lung cancer.10 They found that in this study of over 500 patients and control subjects, only IL-8 levels were associated with lung cancer risk several years before diagnosis. The addition of CRP increased the robustness of biomarker prediction.10 In subsequent studies, including patients and matched controls between 54 and 74 years of age, circulating levels of CRP, serum amyloid A (SAA), soluble tumor necrosis factor receptor-2 (sTNFRII), and monokine induced by gamma interferon (CXCL9/MIG) were associated with lung cancer risk.11
A possibility to measure epigenetic alterations is to detect and quantify CH driven by mutations in epigenetic regulators. CH refers to the premalignant expansion of blood cells derived from a single hematopoietic stem cell.12 While CH is detected in over 10% of individuals aged 60 and older, only 0.5 to 1% will progress to malignant hematopoiesis, including myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML).5 Somatic mutations are well-established drivers of CH, and they most commonly occur in the epigenetic regulators DNMT3A and TET2.5 Both TET2- and DNMT3A-mutated hematopoietic cells have been shown to have a clonal advantage in an inflamed environment13 but also to be associated with increased cell-intrinsic inflammatory signaling, further supporting cloning advantage.14 Thus, this well-characterized interplay between altered epigenetic regulators and inflammation offers an opportunity to further refine our understanding with the ultimate goal of clinical translation.
Stratify cancer patient survival
Nishijima and colleagues studied the association between frailty using the 36-item Carolina Frailty Index (CFI) and neutrophil to lymphocyte ratio (NLR) as an inflammatory marker in cancer patients with a median age of 74 years.15 They found a significant correlation between CFI and NLR; in bivariate analyses, higher NLR was associated with lower instrumental activity of daily living score and prolonged time in the “up and go” test, suggesting an association between frailty and inflammation in older patients with cancer.15
In a prospective multicenter study on more than 1700 patients with a mean age of 71, Ruan et al. suggest the systemic inflammation prognostic score (SIPS) to predict survival in elderly patients with cancer. They determined CRP, the geriatric nutritional risk index (GNRI), advanced lung cancer inflammation index (ALI), and lymphocyte to CRP ratio (LCR) to contribute to the SIPS. The study showed that SIPS is an independent prognostic indicator in elderly patients with cancer, defining three risk groups, with malnutrition in the high-risk group increasing mortality risk.16 The Investigation on Nutrition Status and Clinical Outcome of Common Cancers (INSCOC) study on over 5000 older patients with cancer assessed NLR as the primary marker of inflammation, with frailty being evaluated using the FRAIL scale and primary outcome all-cause mortality. The study found systemic inflammation to be positively associated with frailty. Frail elderly cancer patients with elevated systemic inflammation had a low survival rate.17
Epigenetic markers, especially those associated with an inflammatory signature such as DNMT3A and TET2, are also associated with poor outcome.18
Association between epigenetic changes and inflammation
As age-associated epigenetic changes and inflammaging have been suggested to be associated with cancer, they likely co-occur and potentially cooperate to drive malignant transformation. IL-6 and IL-1β have been shown to lead to increased methylation and subsequently decreased gene expression.19–21 Interestingly, mutations in epigenetic markers that can lead to a premalignant state, such as DNMT3A, ASXL1 and TET2 mutations that cause CH, are also associated with an inflammatory signature and increase cancer risk and are also a risk factor for cardiovascular disease and atherosclerosis.22 These observations suggest an inflammatory state can indicate an underlying epigenetic alteration and vice versa. Monitoring high-risk CH patients can be a valuable measure to detect a malignancy early on or even prevent disease development.
While this is a promising outlook for preventative medicine in the future, it is currently challenging to monitor large numbers of patients over extended periods, and the tools to preventatively treat diseases like leukemia are limited. Preventative drug treatment would require a highly specific mechanism of action against the precancerous cells with low toxicity or side effects in healthy tissues. Epigenetic regulators have recently emerged as promising targets for cancer therapy. They could serve as good candidates for the development of preventative treatment options since some of them, such as histone acetyltransferase KAT7 (HBO1) and menin, a component of the KMT2A histone methyltransferase complex, were shown to specifically target cancer cells.18, 23
Therapeutic targeting of epigenetic regulators and inflammation
Many drugs have been developed to take advantage of the reversible nature of the epigenome. The first generation of epigenetic therapies was developed targeting histone deacetylases (HDACs) with inhibitors such as panobinostat, which is in clinical trials for multiple cancer entities such as multiple myeloma and lymphoma, and demethylating agents such as azacytidine used for myelodysplastic syndrome (MDS), chronic myelomonocytic leukemia and others. Both compound families are highly cytotoxic and while they inhibit epigenetic mechanisms of gene regulation, they do not specifically target malignant cells. Combination treatment of these compounds with chemotherapy or immunotherapy has shown promising effects in certain cancer entities to improve response rates or prevent resistance development.
A newer generation of epigenetic inhibitors targeting epigenetic writers such as histone acetyltransferases or histone methylases, specifically targeting oncogenic chromatin complexes, show promise in preclinical studies.18,24,25
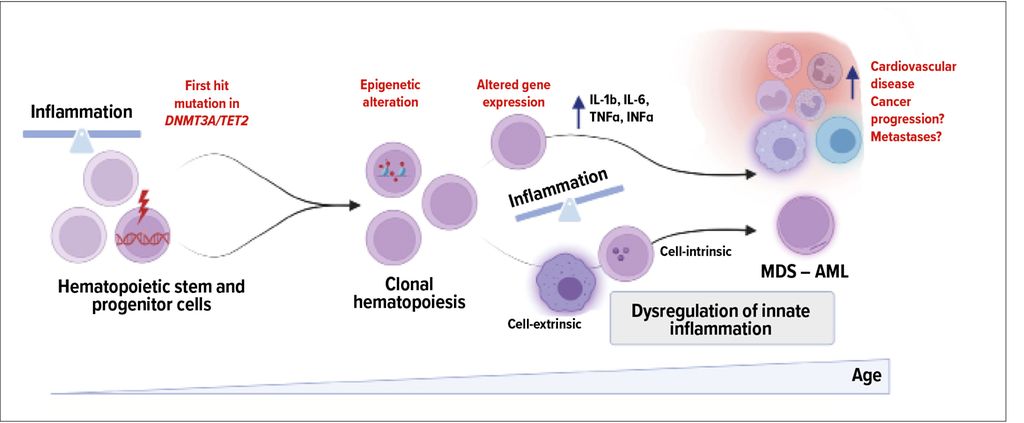
Abb. 1: Simplified model depicting the interplay between altered epigenetics and inflammation in clonal hematopoiesis and beyond driven by DNMT3A or TET2 mutation (created with biorender)
Another recently developed class of inhibitors that emerged are menin inhibitors, which have recently been FDA-approved for treating KMT2A-rearranged leukemia. Rather than targeting the enzymatic function, menin inhibitors function by blocking the interaction of KMT2A with its adapter protein menin, leading to an impairment in the chromatin recruitment of the KMT2A complex.25–27 This strategy was shown to be efficacious in leukemias carrying mutant KMT2A and other leukemia subtypes that rely on wildtype KMT2A.23,28 Inhibiting chromatin binding is a very effective strategy since it disrupts a larger complex rather than the activity of an individual component, which is more easily overcome.
Another approach is to remove epigenetic regulators entirely using degrader compounds. Targeted protein degradation using proteolysis-targeting chimeras (PROTACs) or molecular glues has rapidly developed since the development of the first Brd4 PROTAC in 2015 and is entering clinical trials for a variety of targets and cancer entities.29 While it is still early to see the impact of degraders on patient outcomes, this approach holds great promise for treating cancers in the future.
When thinking about therapeutic targeting of inflammation in malignancies, it has been challenging to identify key disease-initiating or maintaining nodes without impairing essential physiological functions. Tumor-associated macrophages, neutrophils, T-cells, dendritic and stromal cells are part of the central inflammation promoting cells in cancer and produce therapeutically attractive cytokines.30 While these cells contribute to the tumor environment, cell-intrinsic inflammation has also been shown to be a vulnerability in cancer cells.31,32 Widely explored targets are TGF-β within melanoma, renal cell carcinoma, breast cancer, and other cancers.33,34 Another more recent prominent example is targeting the IL-1R-associated kinases (IRAKs) in hematopoietic malignancies.32
Translational perspectives
While no clear guidelines recommend monitoring inflammatory markers for early detection of neoplastic disease, relapse or the estimation of cancer-associated frailty, applying suggested scores on selected patients, can have its right. Cancer should be considered in patients with elevated inflammatory markers as a differential diagnosis.35 As inflammatory and epigenetic changes can be reversible and targetable to prevent or mitigate cancer and treatment-related adverse events, dissecting their translational relevance deserves further research.
Many oncogenic epigenetic mechanisms are relevant across different mutational backgrounds and even across different cancer entities, which expands the impact of these discoveries to a much larger target group. Translating the findings across entities is essential in widening the potential therapeutic advances made in this field.
Challenges, summary, and outlook
The ideal marker should be detectable in peripheral blood, at low cost, routinely offered, and specific. Although retrospective studies might further impact specificity, these requirements are demanding to meet in a real-world patient population. One confounding factor due to the characteristics of the patient population is age, which, as discussed above, alters inflammation as an independent component. Studies suggest that scores tend to be more robust than single markers; in clinical practice, relative variation over time in a specific patient with known disease and associated inflammatory characteristics can have its right to monitor the clinical course long-term. However, more research is required to exploit the full translational potential of epigenetic and inflammatory markers and therapies. Figure 1 summarizes a model of the interplay in the hematopoietic system.
Literature:
1 Hanahan D: Cancer Discov 2022; 12(1): 31-46 2 Rea IM et al.: Front Immunol 2018; 9: 586 3 Caiado F et al.: Blood 2023; 141(8): 886-903 4 Ferrucci L et al.: Blood 2005; 105(6): 2294-9 5 Jaiswal S et al.: N Engl J Med 2014; 371(26): 2488-98 6 Heikkila K et al.: Cancer Causes Control 2009; 20(1): 15-26 7 Coppe JP et al.: Annu Rev Pathol 2010; 5: 99-118 8 Heikkila KS et al.: Eur J Cancer 2008; 44(7): 937-45 9 Il’yasova D et al.: Cancer Epidemiol Biomarkers Prev 2005; 14(10): 2413-8 10 Pine SR et al.: J Natl Cancer Inst 2011; 103(14): 1112-22 11 Shiels MS et al.: J Natl Cancer Inst 2015; 107(10) 12 Zink F et al.: Blood 2017; 130(6): 742-52 13 Cai Z et al.: Cell Stem Cell 2018; 23(6): 833-49 14 Muto T et al.: Nat Immunol 2020; 21(5): 535-45 15 Nishijima TF et al.: JCO Precis Oncol 2017; 1: 1-10 16 Ruan GT et al.: Front Immunol 2023; 14: 936904 17 Zhang Q et al.: Effects of systemic inflammation and frailty on survival in elderly cancer patients: Results from the INSCOC study. Front Immunol 2023; 14: 936904 18 MacPherson L et al.: Nature 2020; 577(7789): 266-70 19 Hmadcha A et al.: J Exp Med 1999; 190(11): 1595-604 20 Maiuri AR, O’Hagan HM: Prog Mol Biol Transl Sci 2016; 144: 69-117 21 Candido S et al.: Perspective on inflammation and cancer relationship. Int J Mol Sci 2021; 22(18) : 10172 22 Jaiswal S et al.: N Engl J Med 2017; 377(2): 111-21 23 Uckelmann HJ et al.: Science 2020; 367(6477): 586-90 24 Baell JB et al.: Nature 2018; 560(7717): 253-57 25 Krivtsov AV et al.:Cancer Cell 2019; 36(6): 660-73 26 Grembecka J et al.: Nat Chem Biol 2012; 8(3): 277-84 27 Issa GC et al.: Nature 2023; 615(7954): 920-4 28 Heikamp EB et al.: Blood 2022; 139(6): 894-906 29 Lu J et al.: Chem Biol 2015; 22(6): 755-63 30 Li L et al.: Int Immunopharmacol 2020; 88: 106939 31 Ellegast JM et al.: Cancer Discov 2022; 12(7): 1760-81 32 Bennett J et al.: Blood 2023; 142(11): 989-1007 33 Morris JC et al.: PLoS One 2014; 9(3): e90353 34 Formenti SC et al.: Clin Cancer Res 2018; 24(11): 2493-2504 35 Watson J et al.: Br J Cancer 2019; 120(11): 1045-51
Das könnte Sie auch interessieren:

Erhaltungstherapie mit Atezolizumab nach adjuvanter Chemotherapie
Die zusätzliche adjuvante Gabe von Atezolizumab nach kompletter Resektion und adjuvanter Chemotherapie führte in der IMpower010-Studie zu einem signifikant verlängerten krankheitsfreien ...

Highlights zu Lymphomen
Assoc.Prof. Dr. Thomas Melchardt, PhD zu diesjährigen Highlights des ASCO und EHA im Bereich der Lymphome, darunter die Ergebnisse der Studien SHINE und ECHELON-1

Aktualisierte Ergebnisse für Blinatumomab bei neu diagnostizierten Patienten
Die Ergebnisse der D-ALBA-Studie bestätigen die Chemotherapie-freie Induktions- und Konsolidierungsstrategie bei erwachsenen Patienten mit Ph+ ALL. Mit einer 3-jährigen ...