©
Getty Images/iStockphoto
Non-alcoholic fatty liver disease
<p class="article-intro">Non-alcoholic fatty liver disease (NAFLD) is one of the most common causes of liver disorder affecting 17–46 % of the general population. When associated with inflammation (non-alcoholic steatohepatitis, NASH) it can lead to the development of liver fibrosis and cirrhosis and is currently one of the leading causes of chronic liver disease.</p>
<hr />
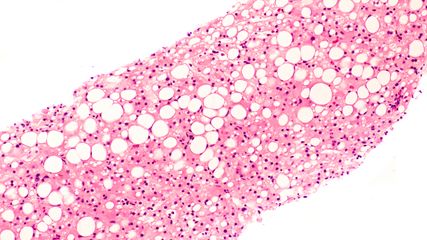
<p class="article-content"><p>NAFLD is considered as the hepatic manifestation of the metabolic syndrome and is seen in low, middle and high-income regions owing to dramatic epidemic proportions of obesity and type 2 diabetes (T2DM) worldwide. Experts are predicting that within the next 10 to 20 years NAFLD related cirrhosis will replace hepatitis C and alcohol as the main cause for liver transplantation. Current areas of active research include screening programs in high-risk groups and the development of new drug therapies to prevent the progression of the disease towards cirrhosis.</p> <h2>Definition and epidemiology</h2> <p>NAFLD is characterized by the accumulation of fat in the liver in more than 5 % of hepatocytes (Fig. 1). It encompasses a spectrum of liver diseases including simple steatosis (non-alcoholic fatty liver; NAFL) and non-alcoholic steatohepatitis (NASH), which is characterized by inflammation and hepatocyte ballooning on the basis of steatosis. Indeed, free fatty acids (FFA) can lead to parenchymal cell injury and trigger inflammation resulting in hepatocyte destruction and fibrogenesis. Hepatic fibrosis is a complex mechanism characterized by the formation and deposition of excess fibrous connective tissue leading to progressive architectural tissue remodeling and increases morbidity and mortality. The diagnosis of NAFLD requires the exclusion of both secondary causes of liver disease including excessive alcohol consumption (defined as a daily alcohol consumption >30 g for men and >20 g for women) and the hepatitis B and C viruses.<sup>1, 2</sup><br /> The burden of disease is impressive as shown by a recent meta-analysis that assessed a global prevalence of NAFLD of 25 % . The highest prevalence rates were reported in South America and the Middle East. Data from this meta-analysis estimated a prevalence of NASH of 1.5 % to 6.5 % in the general population.<sup>3</sup></p> <p><img src="/custom/img/files/files_datafiles_data_Zeitungen_2020_Leading Opinions_Innere (FR)_2001_Weblinks_lo_innere_fr_2001_s47_fig1_medecine_ref_goossens_nafld.jpg" alt="" width="525" height="341" /></p> <h2>Metabolic disorders related to NAFLD</h2> <p>Several studies have demonstrated that NAFLD is strongly related to insulin resistance (IR) and the metabolic syndrome (MetS), defined as the cluster of any three of the following five features associated with IR: impaired fasting glucose (IFG) or T2DM, hypertriglyceridemia, low high-density lipoprotein (HDL)-cholesterol, increased waist circumference and high blood pressure.<sup>1</sup> IR leads to increased lipolysis and release of FFAs which accumulate as ectopic fat, mainly as intramyocellular and hepatic lipids, and can provoke excessive oxidative stress and inflammation.<sup>4</sup></p> <h2>Disease history and progression</h2> <p>Generally, NAFLD is a slowly progressive disease. NAFL as well as NASH can lead to liver fibrosis and cirrhosis. NASH is a more severe disease and time to progressive fibrosis is shorter than in simple NAFL with no inflammation.<sup>5</sup> When compared to alcoholic fatty liver disease (AFLD) NAFLD patients have better prognosis due to lower liver related morbidity and mortality because fibrogenesis in these patients is slower.<sup>6</sup> Advanced liver fibrosis has been shown as being the most predictive factor of mortality in NAFLD suggesting that patients with steatosis should benefit from fibrosis screening with biomarkers or liver elastography.<sup>2</sup><br /> NAFLD is also a risk factor for developing hepatocellular carcinoma (HCC).<sup>7</sup> Prevalence of NALFD related HCC is increasing and the cumulative incidence varies from 0.25 % to 7.6 % at 5 years in patients with advanced fibrosis or cirrhosis.<sup>8</sup> HCC typically arises on the background of cirrhosis. However, about 20 % of cases can develop in a non-cirrhotic liver. Interestingly, NALFD with or without NASH, predispose to HCC.<sup>9</sup> Due to the large number of cases of NAFLD there are currently no cost-effective guidelines available for the surveillance of HCC in these patients.<sup>2</sup></p> <p>It is interesting to note that death from cardiovascular disease (CVD) is more common than liver related death in NAFLD.<sup>10</sup> Results from recent meta-analyses indicate that people with NAFLD are at risk of acute myocardial infarction (AMI) or stroke. Alexander and al. recently collected data on a cohort of 120,000 patients with NAFLD and showed that association between incidental risk of developing a cardiovascular event and NAFLD is lower than estimated previously with a hazard ratio of 1.2.<sup>11</sup> These data suggest that NAFLD is not an independent risk factor of cardiovascular events and that other risk factors should be identified and managed according to usual guidelines.</p> <h2>Current guidelines and treatments</h2> <p>Steatosis should be documented whenever NAFLD is suspected. Practically, patients with obesity and T2DM should have non-invasive screening for NAFLD. Steatosis should be documented by ultrasonography as a first-line diagnostic procedure. Screening serum biomarkers like fatty liver index (FLI) or Steatotest have been developed and can also be used for the detection of liver steatosis. NASH must be diagnosed by liver biopsy.<sup>2</sup><br /> Fibrosis identification and monitoring is the key for follow-up since it is the most important prognostic factor in NAFLD.<sup>12</sup> Combination of non-invasive procedures using biomarkers and elastography can efficiently be used to detect low grades of fibrosis.<sup>13</sup> When advanced liver fibrosis or cirrhosis is suspected liver biopsy should be performed to confirm the diagnosis.<sup>14</sup><br /> There is strong association between lifestyle and NAFLD.<sup>15</sup> Most effective therapies target lifestyle interventions. Weight loss is associated with improved steatosis and IR in T2DM patients. It is also associated with improvement of liver enzymes and histology in obese/overweight patients. Dietary and lifestyle changes towards healthy diet and habitual physical activity are the first line treatment to most of the patients with NAFLD.<sup>2</sup><br /> No drug has yet been approved for the management of NAFLD or NASH. While no firm recommendations have been made, some drug therapies have shown to be beneficial for well selected patients. Generally, pharmacotherapy is reserved for patients with NASH and advanced fibrosis.<sup>2</sup> Insulin sensitizers have been tested and metformin did not show improvement in liver histology in patients with NAFLD compared to placebo after 6 months of treatment.<sup>16</sup> Studies with pioglitazone in non-diabetic patients have shown significant reductions in steatosis, inflammation, and hepatocellular ballooning, as well as improvements in insulin resistance and liver enzyme levels.<sup>17, 18</sup> The PIVENS trial also showed that vitamin E therapy in non-diabetic patients, as compared with placebo, was associated with a significantly higher rate of improvement in NASH.<sup>17</sup><br /> When lifestyle changes and pharmacotherapy fail to reduce and prevent further progression of fibrosis, bariatric surgery can be performed as one option of weight loss.<sup>2</sup> It has demonstrated that it can reduce NAFLD-associated liver injury and histologic lesions of NASH.<sup>19, 20</sup><br /> Future drug therapies target fibrotic pathways. Currently tested molecules include farnesoid X receptor (FXR) agonism (obeticholic acid, nonsteroidal FXR agonists), acetyl-CoA carboxylase inhibition, peroxisome proliferator-activator receptor agonism (elafibranor, lanifibranor, saroglitazar), and fibroblast growth factor (FGF)-21 or FGF-19 activation. Other antifibrotic drug candidates target cell death or inflammation, such as caspase (emricasan) or ASK1 inhibitors (selonsertib), galectin-3 inhibitors and reducing inflammatory macrophage recruitment by blocking chemokine receptors CCR2/CCR5 (cenicriviroc). Efficacious antifibrotic therapies could be available within the next five years.<sup>21</sup></p> <h2>Conclusion</h2> <p>NAFLD is a frequent cause of liver injury and can lead to liver fibrosis and cirrhosis. This disease is strongly linked with the metabolic syndrome. Initial work up includes liver ultrasonography. When suspected, liver fibrosis should be identified by non-invasive procedures or liver biopsy. The current treatment is to manage the metabolic syndrome with lifestyle interventions. Pharmacotherapy is reserved for well selected patients. There are high hopes that future drug therapies targeting fibrogenesis will be available.</p></p>
<p class="article-footer">
<a class="literatur" data-toggle="collapse" href="#collapseLiteratur" aria-expanded="false" aria-controls="collapseLiteratur" >Literatur</a>
<div class="collapse" id="collapseLiteratur">
<p><strong>1</strong> Ratziu V et al.: J Hepatol 2010; 53: 372-84 <strong>2</strong> European Association for the Study of the Liver (EASL), European Association for the Study of Diabetes (EASD), European Association for the Study of Obesity (EASO). J Hepatol 2016; 64: 1388-402 <strong>3</strong> Younossi ZM et al.: Hepatology 2016; 64: 73- 84 <strong>4</strong> Gaggini M et al.: Nutrients 2013; 5: 1544-60 <strong>5</strong> Singh S et al.: Clin Gastroenterol Hepatol 2015;13: 643-54.e9 <strong>6</strong> Haflidadottir S et al.: BMC Gastroenterol 2014; 14: 166 <strong>7</strong> Byrne CD, Targher G: Diabetologia 2016; 59: 1141-4 <strong>8</strong> Dyson J et al.: J Hepatol 2014; 60: 110-7 <strong>9</strong> Desai A et al.: Hepatocellular carcinoma in non-cirrhotic liver: A comprehensive review. World J Hepatol 2019; 11: 1-18 <strong>10</strong> Targher G et al.: N Engl J Med 2010; 363; 1341-50 <strong>11</strong> Alexander M et al.: BMJ 2019; 367: l5367 <strong>12</strong> Ekstedt M et al.: Hepatology 2015; 61: 1547-54 <strong>13</strong> Petta S et al.: Liver Int 2015; 35: 1566- 73 <strong>14</strong> European Association for Study of Liver, Asociacion Latinoamericana para el Estudio del Higado. EASL-ALEH Clinical Practice Guidelines: J Hepatol 2015; 63: 237-64 <strong>15</strong> Zelber-Sagi S et al.: World J Gastroenterol 2011; 17: 3377- 89 <strong>16</strong> Haukeland JW et al.: Scand J Gastroenterol 2009; 44: 853-60 <strong>17</strong> Sanyal AJ et al.: N Engl J Med 2010; 362: 1675-85 <strong>18</strong> Aithal GP et al.: Gastroenterology 2008; 135: 1176-84 <strong>19</strong> Caiazzo R et al.: Ann Surg 2014; 260: 893-8; discussion 898-9 <strong>20</strong> Lassailly G et al.: Gastroenterology 2015; 149: 379-88 <strong>21</strong> Tacke F, Weiskirchen R: Expert Rev Gastroenterol Hepatol 2018; 12: 1143-52</p>
</div>
</p>
Das könnte Sie auch interessieren:
UEGW 2025: Neues aus der Hepatologie
In der Indikation metabolisch bedingte Lebersteatose bzw. Steatohepatitis scheiterten über viele Jahre zahlreiche Therapieversuche. Seit Kurzem stehen erstmals wirksame Therapien zur ...
Fünf Therapien zur Behandlung von MASLD
Mit zunehmendem Übergewicht in der Bevölkerung wird auch die mit metabolischer Dysfunktion assoziierte steatotische Lebererkrankung (MASLD) vermehrt diagnostiziert. PD Dr. Dr. med. David ...
Sonografie der Leber – aktuelle Entwicklungen, quantitative Verfahren und klinische Bedeutung
Der vorliegende Übersichtsartikel fasst aktuelle technische Entwicklungen sowie klinische Anwendungen und Limitationen der Lebersonografie zusammen und diskutiert deren Stellenwert im ...