Multi-stage composite breast reconstruction
Sie sind bereits registriert?
Loggen Sie sich mit Ihrem Universimed-Benutzerkonto ein:
Sie sind noch nicht registriert?
Registrieren Sie sich jetzt kostenlos auf universimed.com und erhalten Sie Zugang zu allen Artikeln, bewerten Sie Inhalte und speichern Sie interessante Beiträge in Ihrem persönlichen Bereich
zum späteren Lesen. Ihre Registrierung ist für alle Unversimed-Portale gültig. (inkl. allgemeineplus.at & med-Diplom.at)
Breast reconstruction after mastectomy is an essential component of modern breast cancer care. Although implant-based reconstruction remains the most commonly used technique, limited soft tissue coverage and long-term implant-related complications can affect durability and patient satisfaction. Composite (hybrid) reconstruction, combining implants with autologous tissue, has therefore emerged to improve tissue quality and enhance the biological integration and longevity of implant-based techniques. In this context, composite reconstruction using repeated autologous fat grafting (AFG) together with implants offers a structured and reproducible approach.
Keypoints
-
Composite (hybrid) breast reconstruction combines implant placement with autologous tissue transfer to improve biological integration.
-
Combining implants with repeated autologous fat grafting (lipofilling) progressively increases mastectomy flap thickness, allowing better coverage.
-
Improved soft tissue coverage enhances a more natural implant placement and provides aesthetic stability.
-
Early results suggest a potential reduction in implant-related complications and secondary refinement procedures.
Concept and rationale
Breast reconstruction following mastectomy is traditionally performed either completely with autologous tissue or with implants. Autologous reconstruction with free flaps provides durable and natural results but requires complex microsurgical procedures, longer operative times, and donor-site morbidity. Implant-based breast reconstruction, although less invasive and widely available, relies on a foreign body and is associated with long-term drawbacks such as capsular contracture, implant displacement, rippling, rupture, and a substantial cumulative risk of revision surgery and implant substitution.
The term composite, or hybrid, breast reconstruction broadly refers to any reconstructive approach combining reconstruction with implants with some form of autologous tissue transfer. Amongst these strategies, the delayed reconstruction combining placement of a tissue expander, repeated sessions of autologous fat grafting and subsequent use of a breast implant is gaining popularity.
Autologous fat grafting to the breast is already widely performed as a secondary aesthetic refinement following breast reconstruction and proven to be safe from an oncological standpoint. In this strategy fat grafting is considered a core component of the reconstructive pathway. By increasing soft tissue thickness over time, the implant becomes better covered, more naturally integrated, and potentially better tolerated in the long term. This approach does not seek to replace flap-based reconstruction but rather to enhance the quality and longevity of implant-based techniques in appropriately selected patients.
Composite breast reconstruction: the general concept
Following mastectomy, a tissue expander is placed, most often in the pre-pectoral plane. After wound healing and progressive expansion, autologous fat grafting is performed around the expander, into the mastectomy flap, through an outpatient procedure. During each fat grafting session, the expander is partially deflated to create space to better accommodate the injected fat, a process defined originally as “reverse expansion” by Stillaert et al.1 This sequence can be repeated several times, depending on patient desire, anatomy and reconstructive goals. Once sufficient soft tissue thickness has been achieved, the expander is replaced with a definitive implant, which benefits from improved coverage and support (Fig.1).

Fig. 1: Multi-stage composite breast reconstruction using repeated autologous fat grafting in pre-pectoral expander-to-implant breast reconstruction: before mastectomy (A); gradual filling of pre-pectoral expander (B); development of thin capsule around expander (2-3 months; C); fat grafting and concomitant expander deflation (D); after final fat grafting and exchange of expander for definitive implant (E)
Soft tissue augmentation and early clinical evidence
Insufficient soft tissue coverage is one of the main determinants of implant-related complications as it increases the likelihood of rippling, visible implants, capsular contracture, and patient dissatisfaction. Moreover, solutions to address thin mastectomy flaps are not free of complications: subpectoral implant placement can lead to breast animation deformity and chronic postoperative pain, while the use of biological or synthetic meshes has been associated with seroma formation and infections. Combining implants and repeated autologous adipose tissue transfer, i.e. fat grafting, in selected patients could offer a reproducible method to address this limitation, biologically increasing soft tissue.
Early clinical results, supported by MR imaging and radiological evaluation, have demonstrated a significant and measurable increase (average increase approaching 92%) in subcutaneous tissue thickness following repeated fat grafting (Fig.2).2 This increase appears to be linear with respect to the number of fat grafting sessions performed and has been documented effective across all body mass index categories, indicating that the technique is not limited to a specific patient morphology. Beyond volumetric gain, these early results suggest encouraging trends regarding the overall complication profile, including reconstructive failure and reoperation rates. Improved tissue quality and coverage may also reduce the need for secondary aesthetic refinement procedures, which are frequently demanded following conventional implant-based reconstruction.
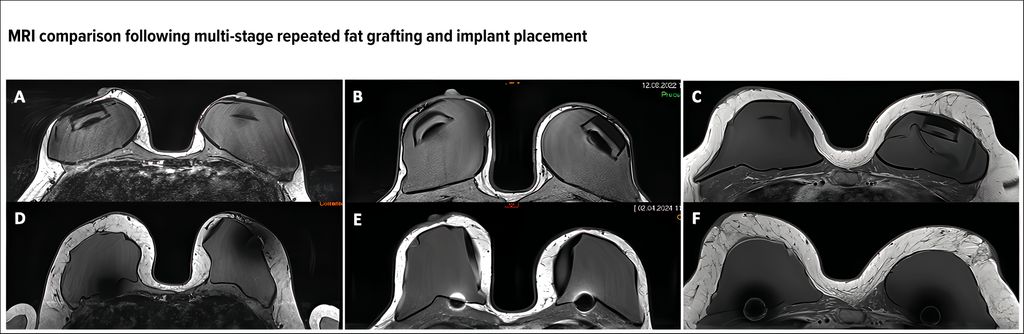
Fig. 2: MRI examinations of a 37-year-old (A), 44-year-old (B), and 46-year-old (C) patient after a bilateral mastectomy sparing both skin and nipple–areolar complexes and pre-pectoral insertion of a breast tissue expander, before repeated sessions of autologous fat grafting of the mastectomy flap and reverse expansion of the expander. D–F: MRI examinations performed 3 months after 3 sessions of autologous fat grafting each and exchange of the expander with a definitive implant. Note the mean gain of tissue thickness in both breasts of 320% (D), 240% (E), and 120% (F)
On the other hand, composite breast reconstruction requires patient compliance and acceptance of a longer multi-stage process compared to standard implant-based approaches. Additionally, although complications directly related to fat grafting are uncommon and usually manageable, oncological follow-up and postoperative imaging requires awareness of fat-related changes such as benign nodules, oil cysts or microcalcifications. Close interdisciplinary collaboration between surgeons, radiologists, and referring physicians remains essential.
Clinical case
A 40-year-old female patient with a history of bilateral subpectoral breast augmentation presented with a left-sided invasive ductal carcinoma (Fig.3A). A skin-reducing mastectomy of the left breast was performed with immediate pre-pectoral placement of a tissue expander (Fig.3B). Given the limited thickness of the mastectomy flaps, a composite reconstructive strategy based on repeated autologous fat grafting was adopted.

Fig. 3: 40-year-old female patient with history of bilateral subpectoral breast augmentation and ductal invasive carcinoma of the left breast T2N0MX, G3 (A). Skin-reducing mastectomy (mastectomy weight: ~470 g) and prepectoral expander insertion (Motiva Flora XMF-62 545 ml) of the left breast prior to 1st fat grafting session (B). 6 months after 3 lipofilling sessions with reverse expansion (210, 280 and 230 ml/breast) and expander to implant substitution on the left breast (Motiva Ergonomix E2SD 380 ml) and implant replacement with pocket change from sub- to prepectoral of the right breast (Motiva E2SF 475 ml) (C)
Three fat grafting sessions were performed over a 10-months period, with injected volumes of 210ml, 280ml, and 230ml, respectively. During each session, partial deflation of the expander was used to facilitate fat integration according to the reverse expansion concept. After completion of the fat grafting phase, the tissue expander was replaced with a definitive implant on the left side, while on the right side implant exchange with pocket conversion from subpectoral to pre-pectoral was performed, achieving bilateral symmetry and stable implant positioning (Fig.3C).
Magnetic resonance imaging performed before and after the reconstructive process demonstrated a progressive and homogeneous increase in soft tissue thickness, particularly in the upper breast quadrants. The postoperative course was uneventful and, at the time of last follow-up (18 months), the aesthetic outcome was judged satisfactory, with no implant-related complications observed.
Conclusion
Composite breast reconstruction based on implants and repeated autologous fat grafting represents a meaningful evolution of implant-based reconstruction. By progressively increasing soft tissue thickness and improving the biological environment surrounding the implant, this approach enhances aesthetic outcomes and may improve long-term reconstructive stability. Early results are encouraging, supporting the role of composite reconstruction as a balanced solution for selected patients, and raising the hope of a more durable implant breast reconstruction.
Literature:
1 Stillaert FBJL et al.: The prepectoral, hybrid breast reconstruction: the synergy of lipofilling and breast implants. Plast Reconstr Surg Glob Open 2020; 8(7): e2966 2 Costa L et al.: Repeated autologous fat grafting significantly increases mastectomy flap thickness in pre-pectoral multi-stage composite expander-to-implant breast reconstruction: exploring the concept of a reverse expansion. J Clin Med 2025; 14(2): 337
Other references available from the authors upon request.
Das könnte Sie auch interessieren:

„Ich habe den schönsten Beruf der Welt“
Mit dem diesjährigen Jahreskongress der Österreichischen Gesellschaft für Plastische, Ästhetische und Rekonstruktive Chirurgie (ÖGPÄRC) in Salzburg hat Prim. Univ.-Doz. Dr. Rupert Koller ...
Minimalinvasive Gesichtsrejuvenation
Die minimalinvasive Gesichtsverjüngung hat sich in den vergangenen Jahren rasant entwickelt. Patienten wünschen sich zunehmend effektive, aber zugleich schonende Methoden, die ohne ...

Neue Wege in der Versorgung grosser Wunden im Kalottenbereich
Grosse Defekte im Bereich der Kopfhaut können dank gesteuerter Geweberegeneration mittels alloplastischer, resorbierbarer Matrix mit dem GREAT-Konzept (Guided Tissue REgeneration by ...