
Detection and treatment of negative symptoms in schizophrenia
Sie sind bereits registriert?
Loggen Sie sich mit Ihrem Universimed-Benutzerkonto ein:
Sie sind noch nicht registriert?
Registrieren Sie sich jetzt kostenlos auf universimed.com und erhalten Sie Zugang zu allen Artikeln, bewerten Sie Inhalte und speichern Sie interessante Beiträge in Ihrem persönlichen Bereich
zum späteren Lesen. Ihre Registrierung ist für alle Unversimed-Portale gültig. (inkl. allgemeineplus.at & med-Diplom.at)
Negative symptoms are among the most disabling and therapeutically challenging features of schizophrenia-spectrum disorders. They contribute substantially to poor functional recovery, impaired quality of life, and enduring social disability, yet they remain systematically overlooked in routine psychiatric care. A rigorous clinical approach requires precise identification of symptom domains, careful distinction between primary and secondary negative symptoms, and a treatment strategy grounded in differential diagnosis and realistic evidence-based interventions.
Keypoints
-
Negative symptoms are a core determinant of long-term disability and poor psychosocial recovery in schizophrenia-spectrum disorders.
-
Their assessment should distinguish primary symptoms from secondary forms related to psychosis, depression, medication side effects, substance use, or social deprivation.
-
Second-generation instruments such as the BNSS and CAINS have improved clinical assessment and better capturing the multidimensional structure of negative symptoms.
-
Treatment remains difficult and effect sizes are often modest, making diagnostic precision and multimodal care essential to improve outcomes.
Why negative symptoms matter
Schizophrenia remains associated with major individual, social, and economic burden.1 Within this broader burden, negative symptoms are particularly important because they are closely linked to poor functional outcome, reduced autonomy, social withdrawal, and diminished participation in everyday life.2,3 In clinical practice, they are often less visible than positive symptoms, yet they frequently determine whether a patient can sustain work, relationships, or meaningful recovery.
Accordingly, modern psychiatry has progressively transitioned from a narrow emphasis on florid psychosis to a dimensional model of schizophrenia, wherein negative symptoms are organized into two principal domains—motivational and expressive impairments—both of which are now considered central therapeutic targets.4–6
Current conceptualization
Negative symptoms are no longer viewed as a single undifferentiated construct. Current models distinguish five consensus domains: blunted affect, alogia, avolition, anhedonia, and asociality.7,8 Factor-analytic work further suggests that these domains cluster at least into two broader dimensions: diminished expression and motivational-pleasure deficits.9
This distinction matters clinically. A patient may present predominantly with reduced emotional expression and poverty of speech, while another may show marked apathy, social disengagement, and reduced anticipation of pleasure. These profiles may differ in functional correlates, neurobiology, and possibly in treatment response.10
Detection: beyond routine observation
Negative symptoms are frequently underrecognized and may be confounded with depression, chronic institutionalization, enduring personality traits, medication effects, or even misattributed to “clinical stability”.11 Yet accurate detection requires more than a general clinical impression. It involves assessing not only observable behavior, but also internal experience, temporal course, and the relationship between symptoms and other psychopathological dimensions.12
Traditional instruments such as the PANSS negative subscale and the SANS remain widely used, but they only partially reflect the current conceptualization of negative symptoms. The EPA guidance therefore recommends complementing first-generation scales with second-generation tools such as the Brief Negative Symptom Scale (BNSS) and the Clinical Assessment Interview for Negative Symptoms (CAINS).3 These instruments better capture the experiential dimension, particularly avolition, asociality, and anhedonia, and help reduce confusion between negative symptoms, functioning, and extrapyramidal effects.
Primary versus secondary negative symptoms
A central issue in both research and clinical care is the distinction between primary and secondary negative symptoms. Primary negative symptoms are considered intrinsic to the illness process. Secondary negative symptoms arise from other causes, including positive symptoms, depression, medication side effects, substance use, and social deprivation.11,13
This distinction is not merely theoretical. It has immediate treatment implications. Social withdrawal may be secondary to paranoid distress; reduced speech and flattened affect may reflect drug-induced parkinsonism; avolition may be related to sedation; anhedonia and withdrawal may be driven by depression rather than by core negative symptomatology.14,15 For this reason, repeated longitudinal assessment is often necessary before concluding that a patient has persistent primary negative symptoms.12
Neurobiological considerations
The neurobiology of negative symptoms remains complex, but motivational deficits have been consistently linked to dysfunction in reward-related circuitry.16 In particular, ventral striatal hypoactivation during reward processing is associated with apathy and motivational impairment rather than with diminished expression per se.17,18 Critically, these reward processing deficits and motivational negative symptoms often persist in stabilized individuals with ongoing antipsychotic treatment.16,19 This highlights that, although current available antipsychotic medication is often effective in treating positive symptoms and the associated striatal dopaminergic abnormalities, it shows little to no effect in ameliorating motivational negative symptoms.20,21
In this regard, numerous computational and neuroimaging studies have shown that negative symptoms cannot be simply explained by the same dopaminergic dysfunction hypothesized for positive symptoms.22 Together with the multifaceted nature of negative symptoms and various contributing clinical and environmental factors, this suggests a more complex and neurobiological framework.10
Treatment of primary negative symptoms
The treatment of primary negative symptoms remains an area of partial therapeutic impasse. No intervention has shown large, consistent, and universally generalizable effects, and the evidence base remains limited by heterogeneous definitions, short trial durations, and insufficient separation of primary and secondary symptoms.3,11
Current guidance nevertheless supports several pragmatic principles (Fig. 1). First, if clinically feasible, second-generation antipsychotics are generally preferred over first-generation agents when negative symtoms are prominent, partly because they are less likely to worsen secondary negative symptoms through excess of D2 blockade and extrapyramidal adverse effects.5,24 Second, antidepressant augmentation may be considered in selected cases, although its effects appear weak to modest and interpretation remains complicated by overlap with depressive symptoms.15
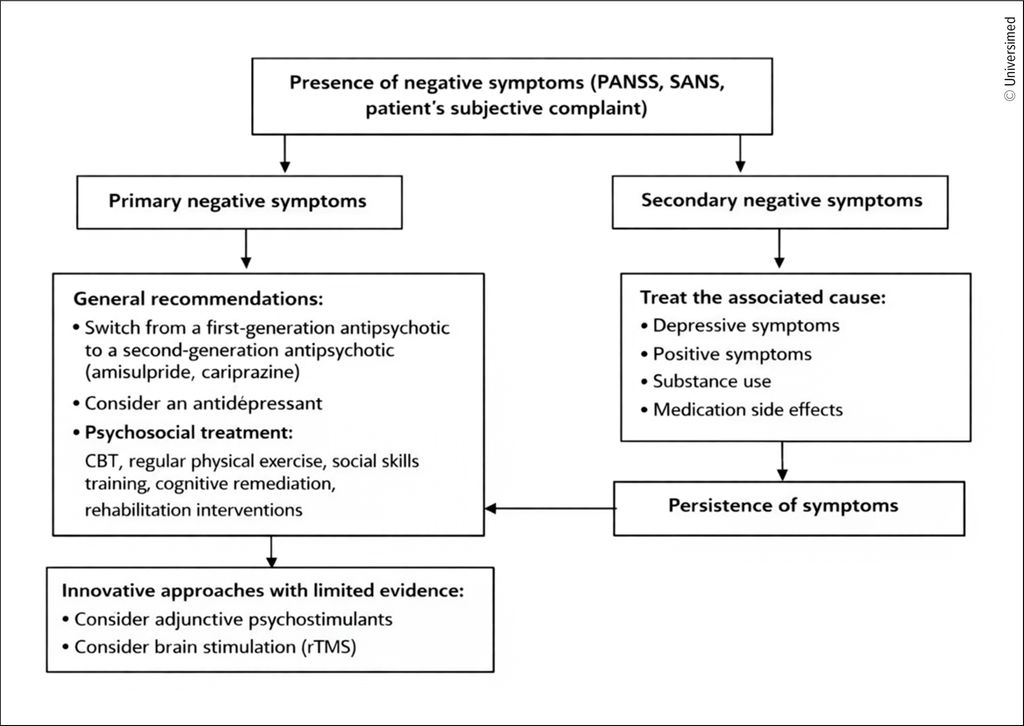
Fig. 1: Clinical assessment and treatment of negative symptoms
Interest has also emerged in pro-dopaminergic strategies, as pro-dopaminergic agents may reduce negative symptoms in selected contexts, although the evidence is not strong enough to justify broad routine use.25,26
Non-pharmacological psychosocial interventions deserve particular emphasis. Social skills training remains the non-pharmacological intervention with the most established evidence.27 Exercise-based intervention is also a promising adjunctive strategy, with report of beneficial effects on negative symptoms in a meta-analysis of randomized trials.28 Meditation-based and mind-body approaches have also shown some signal, although the data remain limited and should be interpreted cautiously.29 In addition, cognitive-behavioral therapy,30 cognitive remediation, and structured rehabilitation approaches may be useful, particularly when integrated into a broader recovery-oriented treatment plan.
Treatment of secondary negative symptoms
Treatment of secondary negative symptoms begins with identifying and treating the underlying cause11 (Fig.1). If symptoms are secondary to persistent psychosis, the primary task is better control of psychotic symptoms. If they reflect depressive pathology, mood symptoms must be specifically assessed and treated. If any signs of antipsychotic side effects (e.g. sedation, parkinsonism) are present, clinicians should reconsider dose, tolerability, and the possibility of switching to a better tolerated regimen.24 Substance use also deserves careful evaluation. For instance, cannabis is highlighted as a clinically relevant contributor to motivational and social impairment.31 More broadly, the assessment of secondary negative symptoms should always include a substance history, because toxic effects, withdrawal, and lifestyle disruption may all contribute to an apparent negative-symptom picture.5
Conclusion
Negative symptoms should not be considered secondary concerns in schizophrenia-spectrum disorders. They are central determinants of long-term disability, poor real-life functioning, and incomplete recovery. Their management begins with better detection, and better detection begins with improved phenomenology, better measurement, and careful differential diagnosis. Although current treatments remain challenging and effect sizes are modest, a structured clinical approach combining precise differential diagnosis with pharmacological, psychosocial, and rehabilitative interventions offers the best available pathway toward meaningful symptom reduction and functional recovery.
References:
1 Chong HY et al.: Global economic burden of schizophrenia: a systematic review. Neuropsychiatr Dis Treat 2016; 12: 357-73 2 Fervaha G et al.: Motivational and neurocognitive deficits are central to the prediction of longitudinal functional outcome in schizophrenia. Acta Psychiatr Scand 2014; 130(4): 290-9 3 Galderisi S et al.: EPA guidance on assessment of negative symptoms in schizophrenia. European Psychiatry: J Assoc Europ Psychiatrists 2021; 64(1): e23 4 Correll CU, Schooler NR: Negative symptoms in schizophrenia: a review and clinical guide for recognition, assessment, and treatment. Neuropsychiatr Dis Treat 2020; 16: 519-34 5 Galderisi S et al.: EPA guidance on treatment of negative symptoms in schizophrenia. Eur Psychiatry 2021; 64(1): e21 6 Strauss GP, Cohen AS: A transdiagnostic review of negative symptom phenomenology and etiology. Schizophr Bull 2017; 43(4): 712-9 7 Kirkpatrick B et al.: The NIMH-MATRICS consensus statement on negative symptoms. Schizophr Bull 2006; 32(2): 214-9 8 Strauss GP et al.: Reconsidering the latent structure of negative symptoms in schizophrenia: a review of evidence supporting the 5 consensus domains. Schizophr Bull 2019; 45(4): 725-9 9 Strauss GP et al.: Deconstructing negative symptoms of schizophrenia: avolition-apathy and diminished expression clusters predict clinical presentation and functional outcome. J Psychiatr Res 2013; 47(6): 783-90 10 Bègue I et al.: Pathophysiology of negative symptom dimensions of schizophrenia - Current developments and implications for treatment. Neurosci Biobehav Rev 2020; 116: 74-88 11 Kirschner M et al.: Secondary negative symptoms - a review of mechanisms, assessment and treatment. Schizophr Res 2017; 186: 29-38 12 Del Goleto S et al.: Recovery-oriented standardized assessment in psychotic disorders. Rev Med Suisse 2025; 21(931): 1658-62 13 Mucci A et al.: Primary and persistent negative symptoms: concepts, assessments and neurobiological bases. Schizophr Res 2017; 186: 19-28 14 De Pieri M et al.: Negative symptoms and their associations with other clinical variables and working memory across the schizophrenia spectrum and bipolar disorder. Schizophr Bull Open 2024; 5(1): sgae024 15 Helfer B et al.: Efficacy and safety of antidepressants added to antipsychotics for schizophrenia: a systematic review and meta-analysis. Am J Psychiatry 2016; 173(9): 876-86 16 Stepien M et al.: Investigating the association of ventral and dorsal striatal dysfunction during reward anticipation with negative symptoms in patients with schizophrenia and healthy individuals. PloS One 2018; 13(6): e0198215 17 Kirschner M et al.: Ventral striatal dysfunction and symptom expression in individuals with schizotypal personality traits and early psychosis. Schizophr Bull 2018; 44(1): 147-57 18 Waltz JA et al.: Motivational deficits in schizophrenia are associated with reduced differentiation between gain and loss-avoidance feedback in the striatum. Biol Psychiatry Cogn Neurosci Neuroimaging 2018; 3(3): 239-47 19 Moran EK et al.: From neuroimaging to daily functioning: a multimethod analysis of reward anticipation in people with schizophrenia. J Abnorm Psychol 2019; 128(7): 723-34 20 Nielsen MO et al.: Improvement of brain reward abnormalities by antipsychotic monotherapy in schizophrenia. Arch Gen Psychiatry 2012; 69(12): 1195-204 21 Wulff S et al.: The relation between dopamine D(2) receptor blockade and the brain reward system: a longitudinal study of first-episode schizophrenia patients. Psychol Med 2020; 50(2): 220-8 22 Howes OD, Shatalina E: Integrating the neurodevelopmental and dopamine hypotheses of schizophrenia and the role of cortical excitation-inhibition balance. Biol Psychiatry 2022; 92(6): 501-13 23 Husain M, Roiser JP: Neuroscience of apathy and anhedonia: a transdiagnostic approach. Nat Rev Neurosci 2018; 19(8): 470-84 24 Sabe M et al.: Antipsychotics for negative and positive symptoms of schizophrenia: dose-response meta-analysis of randomized controlled acute phase trials. NPJ Schizophr 2021; 7(1): 43 25 Luykx JJ et al.: Long term safety of ADHD medication in patients with schizophrenia spectrum disorders. Mol Psychiatry 2025; 30(10): 4859-67 26 Sabe M et al.: Cannabis, nicotine and the negative symptoms of schizophrenia: systematic review and meta-analysis of observational studies. Neurosci Biobehav Rev 2020; 116: 415-25 27 Turner DT et al.: A meta-analysis of social skills training and related interventions for psychosis. Schizophr Bull 2018; 44(3): 475-91 28 Sabe M et al.: Cannabis, nicotine and the negative symptoms of schizophrenia: systematic review and meta-analysis of observational studies. Neurosci Biobehav Rev 2020; 116: 415-25 29 Rao NP et al.: Add on yoga treatment for negative symptoms of schizophrenia: a multi-centric, randomized controlled trial. Schizophr Res 2021; 231: 90-7 30 Favrod J et al.: Improving pleasure and motivation in schizophrenia: a randomized controlled clinical trial. Psychother Psychosom 2019; 88(2): 84-95 31 Sabe M et al.: Physical exercise for negative symptoms of schizophrenia: systematic review of randomized controlled trials and meta-analysis. Gen Hosp Psychiatry 2020; 62: 13-20
Das könnte Sie auch interessieren:

Das Endocannabinoidsystem als potenzieller therapeutischer Ansatzpunkt bei Substanzkonsumstörungen
Das Endocannabinoidsystem (ECS) spielt eine zentrale neuromodulatorische Rolle bei der Regulation von Stress- und Belohnungsprozessen. Eine gezielte pharmakologische Manipulation des ECS ...

«Subjective cognitive decline» – was es bedeutet und wie wir handeln sollten
Viele Patientinnen und Patienten berichten früh über Gedächtnisveränderungen – bei unauffälliger Testdiagnostik. Dieses Stadium, die subjektive kognitive Beeinträchtigung («subjective ...

Esketamin und Psilocybin in der Psychiatrie – ein Paradigmenwechsel?
Esketamin und Psilocybin stehen für neue interventionelle Behandlungen in der Psychiatrie. Sie gelten als schnell wirksame Verfahren mit hohem Potenzial, aber gehen mit methodischen, ...